📍 Published in JMIR Extended Reality, our recent case series explores something simple yet complex:
Can Virtual Reality (VR) be used in real-life clinical workflows before surgery, not as a study add-on, but as part of actual care?
This #SundayResearchDive brings you the story behind the pilot: what worked, what we learned, and what we’ll change next.
🎥 Behind the Scenes: Recording the 360º Hospital Walkthrough
Before testing the intervention, we co-created a 360º video showing the real steps of a patient’s journey on surgery day: from check-in to the operating theatre.
📋 The script was co-written with clinical and communication teams and filmed on-site during regular shifts. To avoid disrupting workflow, filming started early in the morning, capturing real hospital dynamics before surgical activity began.
🩺 Nurses and doctors appeared in the video playing their real-life roles, not actors, but actual professionals from our hospital.
💬 One unexpected outcome? Several patients recognized the staff from the video during their surgical admission. This created a surprising sense of familiarity and reassurance, turning a sterile, stressful moment into something more human and grounded.
🔬 The Core: Learning if VR “Fits” the Hospital Workflow
🎯 This wasn’t an efficacy trial. It was a usability and feasibility study.
Could we integrate Virtual Reality (VR) into routine outpatient surgery workflows?
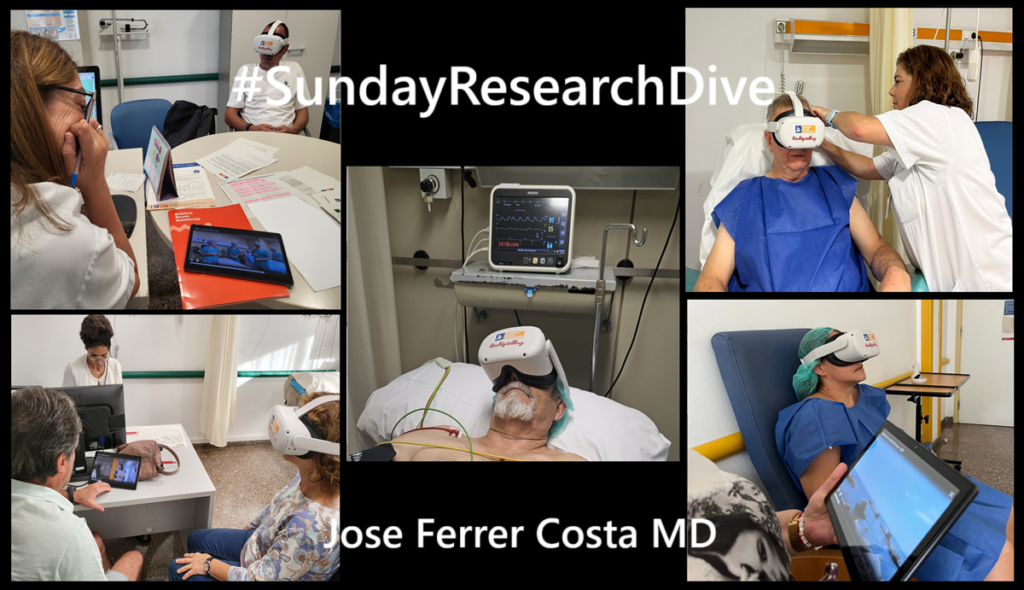
🩺 10 patients | 🕶️ 3 VR interventions | 👨⚕️ Real clinical context
1️⃣ Informative 360º video (preanesthetic visit)
Shown individually during the ambulatory anesthesia consultation. Patients viewed the immersive hospital walkthrough using a VR headset, while caregivers followed the content on a connected tablet.
2️⃣ Mindfulness meditation (preparation ward)
Delivered once patients were admitted. The session combined beach visuals with a guided meditation recorded by a mindfulness-trained GP. It was the easiest stage to integrate and widely described as calming.
3️⃣ Immersive relaxation (preanesthesia room)
Offered during IV line placement. The underwater scene with music aimed to reduce tension, but time pressure and patient stress made this the most challenging to implement.
📲 The headset was connected to a tablet, no internet needed, but still requiring local pairing. This dependency remains a barrier in Wi-Fi-limited clinical spaces and is a key point for future optimization.
👩⚕️ The intervention was delivered and evaluated by 3 nurses and 1 anesthesiologist, who rated usability as high and provided key suggestions for improvement.
📊 What We Measured (and Why)
Although this was a usability study, we also explored how patients responded – emotionally and physiologically – within the actual surgical workflow:
✔️ Usability – Could patients and professionals use VR comfortably and meaningfully?
✔️ Physiological/Anxiety Markers – Were there visible signs of calming effects, even in this small sample?
✔️ Medication Use – As an exploratory observation, did VR help reduce reliance on sedatives?
✅ Key Observations: Promising Signals in a Routine Clinical Context
With the VR intervention in place:
- All 10 patients completed the first two stages
- 6 patients completed all three VR stages
- None of these 6 received midazolam before surgery
- Only 4 out of 10 received diazepam after the mindfulness session
💡 In our setting, the use of sublingual diazepam in the preparation ward and IV midazolam in the preanesthesia room is standard practice to manage preoperative anxiety.
📉 Anxiety levels (STAI-6) dropped significantly after the mindfulness session (p = 0.011), and although they rose slightly in the preanesthesia room, they remained below baseline levels, despite the high-stress situation and in the absence of pharmacological anxiolysis.
✅ Usability scores were high
👤 Patients: 89.1
👩⚕️ Professionals: 80.5
⚠️ This study was not designed to demonstrate efficacy, but these exploratory signals suggest that a structured, non-pharmacological approach using VR may help reduce the need for sedatives – a key hypothesis for future trials.
💡 What the Paper Doesn’t Say (But You Should Know)
🔧 Implementation logistics were key.
- The 360º video was well received, but showing it individually was time-consuming. We’re now exploring more scalable options, like projecting it on a standard screen in the waiting room.
- The mindfulness session was, by far, the easiest to integrate. For patients not scheduled early, it helped reduce tension and made the wait feel more manageable.
- In the preanesthesia room, delivering the final relaxation session was more difficult. Time was tight, and stress levels were high. One of the nurses suggested pre-selecting patients more likely to benefit, and also offering the experience on demand, when anxiety is visible or delays occur, making the patient wait longer.
🎯 Bottom Line:
This study wasn’t about proving VR works. It was about testing whether it can be safely and meaningfully implemented in real clinical workflows.
The answer? Yes, under the right conditions.
We now have:
✔️ A tested 3-stage VR intervention
✔️ Real user feedback
✔️ A roadmap for workflow adaptation
📘 Read the full study here: https://www.liebertpub.com/doi/10.1089/jmedxr.2024.0061
#SundayResearchDive #PreoperativeCare #VirtualReality #Usability #PerioperativeMedicine #DigitalHealth #SurgeryInnovation
This article was originally published on vrforhealth